

“'Cos things break, don't they?” – Mr. Dino Vercotti
This post is about the unprecedented public hospital crisis in France, which has been exacerbated by the COVID-19 pandemic but long pre-dates it.
Before getting started, however, I’m going to run you through a recent personal crisis.

That’s me, stumbling forward (aka “trail running”) high above the Mediterranean late last May, on the rim of a limestone cliff completely denuded of soil by umpteen million years of mistral winds from the north.
David Flynn took the photograph with his iPhone, barely slowing as he turned. He’s a man of many qualities, the most pertinent in this context being: competitive trail runner, half my age, ten times fitter; properly shod.
“You should borrow a pair of my trail shoes,” he said at dinner in Marseille the night before, looking down at my worn-out Nikes.
Nah.
A few seconds after he snapped the photo above, I snapped this.
It turns out that “calanque”, an old provençal word for an inlet surrounded by steep stone walls, is, also, funnily enough, precisely the sound that my funny bone makes when it lands and fractures on jagged rocks. Ka-lonk! The inimitable sound of three bone fragments calanquing off the upper end of the left ulna, the projecting olecranon, the remaining stumped piece exposed beneath the deep gash, the snapped-off bits floating in a loose skin sack leaking blood on the blinding white stone and the stunted scrub growing out of its cracks on both sides of the trail: red drops on the fragrant green leaves of juniper, sage and myrtle shrubs, spraying splashes in great red lashings on the quivering purple rushroses, which, David had just told me, just before my old-geezer fall, blossom and die in a single day.

Fortunately, David took no pictures of our scrambling descent through cascades of loose rock into the calanque, blood blossoming from the gash, red clouds in crystal hues of blue water. No pictures, either, thankfully, of the steady trail of blood marking every teetering lurch of the hike back up and out. Nor of my t-shirt, my shoes, the passenger seat, or the metronomic drips on the floor of the emergency ward.

“Did you hit your head?” the admitting nurse asked. “Do you need a painkiller?”
Nah.
Which put me at the far end of the triage line. Stoicism, it seems, has no pragmatic value in an emergency ward. Nor does steady blood loss. Wincing, whining, moaning, fainting, these alone get results.
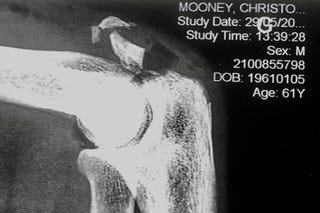
Sixty minutes later, however, I was x-rayed. A half hour after that, examined by a surgical intern. Ninety minutes more, intravenously infused with antibiotics, cleaned, stitched, bandaged, vaccinated against tetanus and shown the door, armed with a sling, prescriptions, recommendations, and a three-page hospitalisation report.
Imagine our surprise then, when, at the pharmacy, we discovered that, having entered the hospital a 61-year-old male (whose first name, French health insurers have always insisted, despite repeated corrections, is Christophe, not Christopher) I miraculously exited a 19-year-old male named Mohammed. Who, somehow, having had the serendipitous misfortune of calanquing a left elbow in the same manner and at the same time and in the same part of the world that Christophe(r) had calanqued his, then assumed his identity. And he, presumably, mine. Or his. Ours.
Something like that.
What are the chances? Probably pretty high.
The nurse who tenderly held my head and gave me nitrous-oxide suckle during my bone-cleaning session told me that she had seen more than 100 patients already that day, and would continue apace, seeing roughly 25 an hour. “Ten more than before the pandemic,” she said. “And tourist season’s coming. The number will double.”
Since the beginning of the pandemic, La Timone’s emergency ward has gone from 30 emergency physicians to 16, and half its nurses have either quit nursing or gone into the private sector.
Normally, at the end of June, new graduates from the country’s nursing schools (three years of study post-baccalaureate) bring in fresh reinforcements. Last year, however, only 30% of the graduating class joined the public.
“Everyone’s already overworked,” she said, “and everyone’s quitting, and no one’s filling the vacancies.
“Who wants to work in a public emergency ward? The pay is lousy, and the stress is intense.”
Night shifts, weekends. Extended hours. Management begging them to forego vacations and leaves of absence.
Until 2010, theirs was considered a “painful” profession, thus eligible for pension at 57. Today, they have to wait till they are 62. Soon, if Macron’s reforms go through, it will be 65.
“A hospital bed is a parked taxi with the meter running.” – Groucho Marx
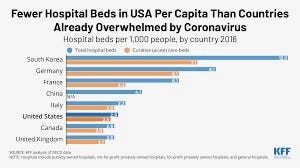
Since 2000, more than 80,000 French public hospital beds have been closed, a 25% drop from 20 years ago. Intensive care unit beds, however, so vital during the pandemic, increased 5% between 2013 and 2019. And France still has 5.7 beds per 1,000 inhabitants, compared to 2.8. in the US, 2.5 in Canada, and 2.3 in the UK.
Yet the number of available hospital beds in France has been dropping every year, as hospitals, following government budget-control requirements and facing increases in activity and an ageing population (and an ongoing pandemic) try to meet objectives imposed upon them by the French Ministry of Health: to keep budget increases at roughly 2% a year, instead of the 4% that Social Security estimates they yearly require. The system, called ONDAM, has been around since the 1980s, when hospital costs started to sharply spike (reaching around 55% of all health expenditures in 1982). It imposes a global budget for public hospitals (and all forms of other publicly funded health-care), which is voted on annually by the French parliament.
The system functioned well at the start, successfully slowing hospital expenditure growth rate, which dropped from an annual average rate of 8% before 1983 to 4% since.
But in recent years, Ministry of Health has doubled down on France’s public hospital expenditure growth rate.
For the 2022 hospital budget (97 billion euros), the difference between what the hospitals require to operate (4% more than 2021) and what ONDAM was willing to give them (1.9%) is roughly 1.8 billion euros.
To achieve these savings, the Ministry of Health uses an activity-based costing mechanism (ABC) that, to make public hospitals “profitable”, lowers the price of operations to keep the “natural budgetary increase” of 4% at 2%. Therefore, a hospital that carries out the same activities from one year to the next will receive less money each year, since the costs of those activities have been lowered. And so on, a vicious circle of increasing activity for less return.
So, naturally, corners are cut.
Infamously, a 99-year-old woman remained on a stretcher at La Timone’s emergency ward for more than 19 hours before a bed was found for her. Other patients waited 36 hours in a corridor. Twelve to 24 hour waits were not uncommon.
And this was in 2019, before COVID-19. Beds were already lacking. Nurses were not only scarce, but many of those still working were on strike, fed up with being the worst paid in Europe.
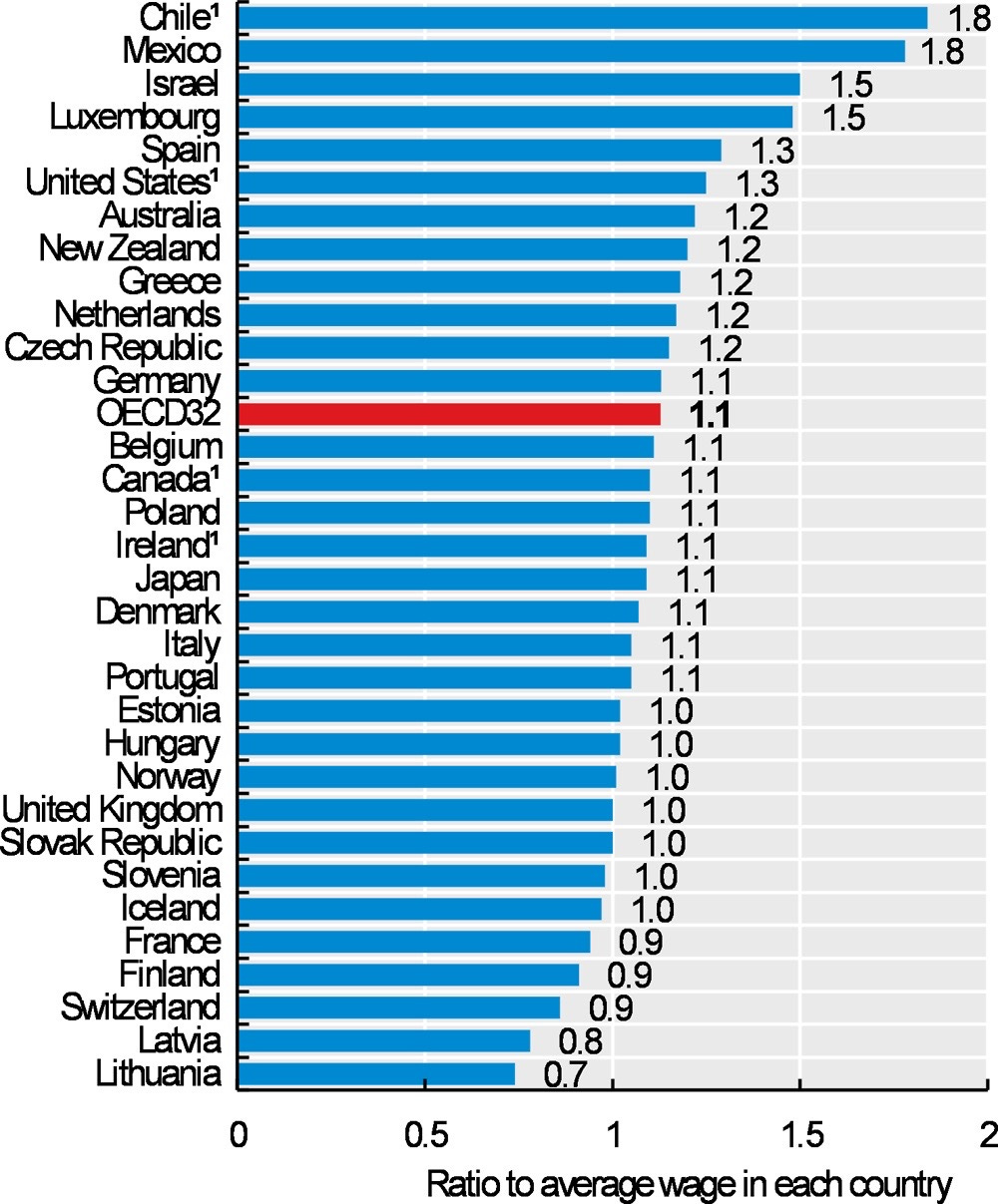
According to the most recent figures I could find (DREES, 2018), the median monthly salary of a nurse at a public hospital is 2,258 euros net, and only 1,774 euros net for a caregiver.
In terms of purchasing power parity (PPP), French nurses earn 20% less than their United Kingdom counterparts, 26% less than German nurses and 40% less than Belgium nurses. Those in the United States make 56% more, which explains why several thousand foreign nurses flock to the States every year.
Of course, France is not the only European country experiencing a healthcare crisis.
Germany’s emergency wards are short 8,000 doctors and 14,000 nurses. It takes on average two months to see a specialist in Spain, and 700,000 Spanish patients have been waiting six months for surgery – 140,000 of them for life-saving operations.
It’s never taken me more than a week to see a specialist.
My GP sent me for a heart scan recently. It took four days to get an appointment. My experience (all good!) sent a friend to do likewise. Four stents later, briskly programmed, prefaced and followed by all manner of scans and followup, and he is swimming a kilometre every day.
Because of the severity of his illness, his insurance was ramped up to 100% coverage.
Meaning he paid nothing.
After my ka-lonk, a nurse came to my home and changed my bandages every two days for two weeks. Out of pocket, nada.
My daughter once reported double vision; two days later she had an MRI, for a negligible fee.
Etcetera.
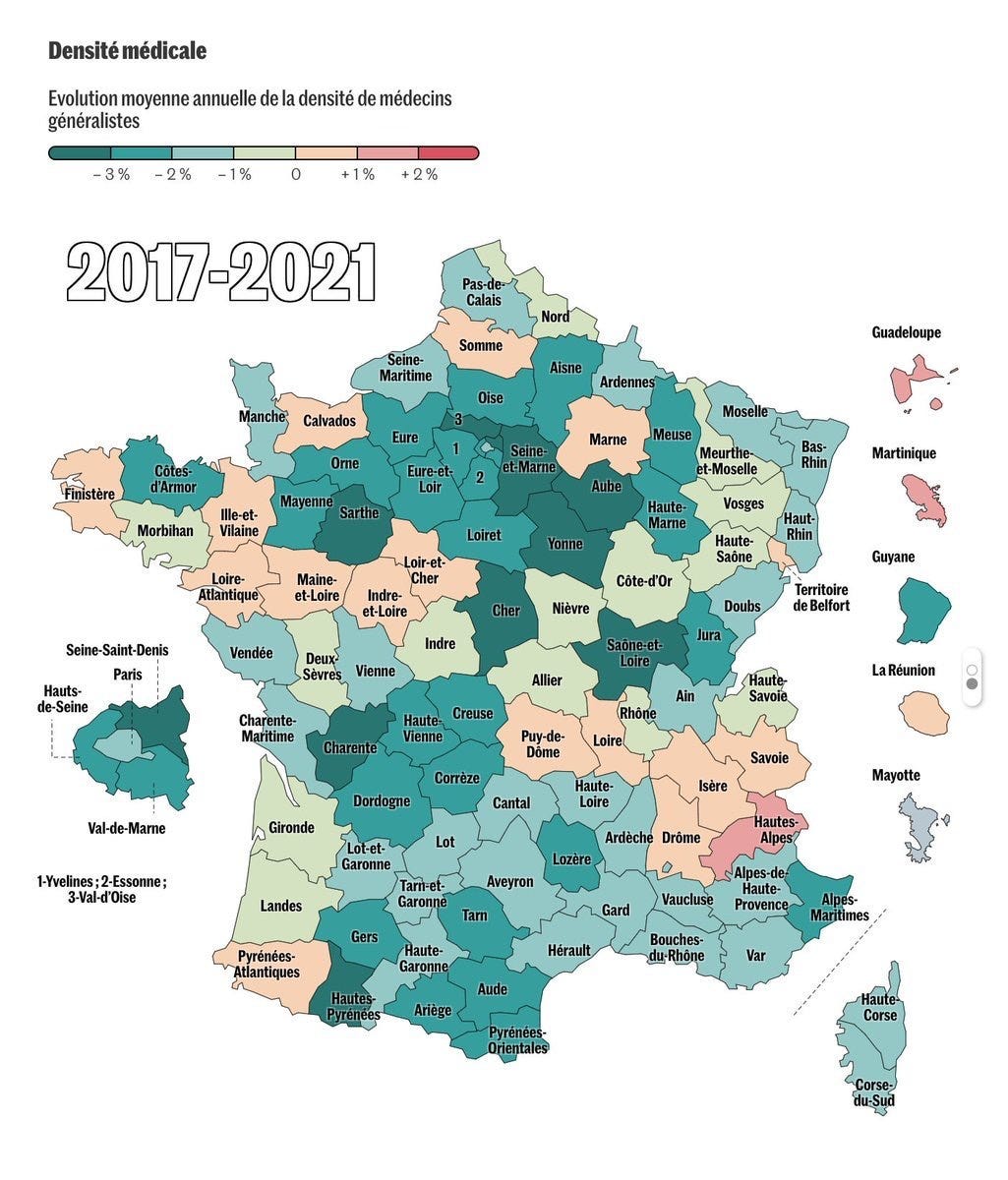
Of course, we live in Paris, not yet a region whose population has inadequate access to healthcare. Those so-called “medical deserts” are still mainly in rural areas, but increasingly in urban and suburban ones. GPs there are scarce, specialists scarcer, and emergency wards have reduced their opening hours or closed entirely.
But, still…
Understandably, the gradual grinding down of the French economic exception, especially in healthcare and education, is worrisome to many of the country’s citizens (and residents like me).
François Braun, an emergency doctor, the former head of the Samu-Urgences de France, the emergency ambulance union, was appointed Health Minister on July 4th. Among his first statements: “Our health system is sick, our health system is suffering, we have to recognize that."
What he’ll do about it, or can do about it, remains to be seen. It is still too early to tell whether the government’s much-vaunted “mission flash” for summertime emergencies and unscheduled care, unveiled July 11, is just in the pan. So far, it seems focussed on telling people to call 15, the emergency service number, before showing up at an emergency ward, or a new hotline number set up to help people through the heatwave.
Meanwhile, COVID-19 numbers continue to spike, and hospital workers are preparing for the worst, and for a big walk-out in September, should no relief come sooner.
Understandably, too, minor snafus like Mohammed’s and my identity-swap at La Timone will happen.
And that no one once checked my vitals. I was convinced for a few days that I had received his treatment (cleaning, bandage, paracetamol) and he mine (extensive surgery, cast, more antibiotics, anti-inflammatories and codeine-laced paracetamol). But the intern’s work was declared top notch by no less than the director of orthopaedics at Hôpital Saint-Antoine in Paris, who saw me less than a week later. And gave me a prescription for unlimited physiotherapy.
And then the bill from La Timone came.
19.60 euros.
ouch! I hope your arm is healing quickly. Thanks for this piece. These are unfortunately familiar statistics, echoed here in BC with health care workers including doctors and nurses leaving in droves...
Wonderful! I’m reading this, but can still hear your voice. Love the writing!